



In today’s culture, schools do more than just educate. They are outreach centers, health care providers, and community leaders who are integral to connecting families to services. Much of this is rooted in the development of schools as health care providers and Medicaid outreach organizations.
One of the predominant Medicaid reimbursement programs that schools participate in as a health care provider is referred to as fee-for-service (FFS) claiming. Also known as direct service or interim claiming, this is the process by which schools get reimbursed for health services provided to some students.
The evolution of fee-for-service claiming
School-based health services expanded beyond the school nurse in 1975, when the first iteration of what is now referred to as the Individuals with Disabilities Education Act (IDEA) was enacted. This act mandated equal access to a general education for all students, raising the standard for student rights across the country and creating a mandate for Individualized Education Programs (IEPs) for students with disabilities. As part of that standard, regulations stipulated that any student with a disability that affected their ability to receive a general education should be treated for that disability by the school, thereby allowing that student a Free Appropriate Public Education (FAPE).
With this act, schools evolved to become health care providers, hiring occupational therapists to help students with dexterity issues, speech-language pathologists to work with students with language comprehension or aphasia, and psychologists and behavioral therapists and counselors to support student mental health.
One hitch, however: funding for this mandate was not provided.
In 1988, an amendment was passed that allowed school districts to enroll as Medicaid providers to support the delivery of services mandated in students’ IEPs, plunging school districts into the world of Medicaid claiming for the first time. Understanding the FFS Medicaid program and its complexities will help any school district participating in this program to maximize their services and revenue.
Federal and state regulations
How the fee-for-service program works in any state is a mix of both federal guidance and state regulations. At the federal level, the Centers for Medicare & Medicaid Services (CMS) has defined the scope and best practices for Medicaid in schools through a technical assistance guide and other publications. The types of services and programs that are potentially billable are outlined at this level. Within the CMS’s guidelines, states make the ultimate decision on multiple levels.
Service types that can be claimed through fee-for-service
At the federal level, allowable service types include:
“Physicians’ services and medical and surgical services of a dentist, medical or other remedial care provided by licensed practitioners, clinic services, dental services, physical therapy, occupational therapy, and services for individuals with speech, hearing and language disorders, diagnostic services, preventive services, rehabilitative services, transportation services, nurse practitioner services, private duty nursing services, personal care services, family planning services.”
Any given state might choose only a portion of service types within this list to include in their program. For example, in many states, personal care services and transportation are not billable through the FFS program.
Rate and unit type of each allowable procedure for each service
Medicaid is a federal and state matching program, meaning the federal government supplies at least 50% of the funding and potentially more based on state need. Because school districts are funded directly by state taxes, schools only receive the federal portion of any fee submitted for payment, referred to as the Federal Medical Assistance Percentage (FMAP) rate. So, if a service is billed for $10, a school district will receive $5 or more, depending on the FMAP rate in each state.
You may enjoy this hand-picked content:
Although Medicaid revenue for school districts is only funded through the federal match of the Medicaid program, states are the administrators of the program, so they decide the rate of payment for service. Each state publishes a fee schedule that identifies the rate for each procedure a therapist can perform, the rate associated to that procedure, and the unit of measurement. Rates differ widely across various states. For example, in Texas, an evaluation of speech fluency has a rate of $2.93, and in Nevada the same procedure has a rate of $96.66.
The exact licensures that can bill for services in the state
Because medical licenses and certifications are state based, states also decide which type of license, certification, or qualification is required within each service type for a service to be billable. This varies widely across states. In Virginia, for example, assistants of multiple service types can bill services. In Missouri, for physical and occupational therapy, only therapists who are licensed can bill services.
Record keeping and documentation requirements for services
As the administrators of the Medicaid program, state offices also conduct the majority of audits and define which records must be kept on file and what documentation must be conducted to support the billing of services. The requirements for service documentation, timing of service documentation, and records like IEP documents and doctors’ orders are all under state purview and defined in state billing manuals.
Enrollment and enrolling entities
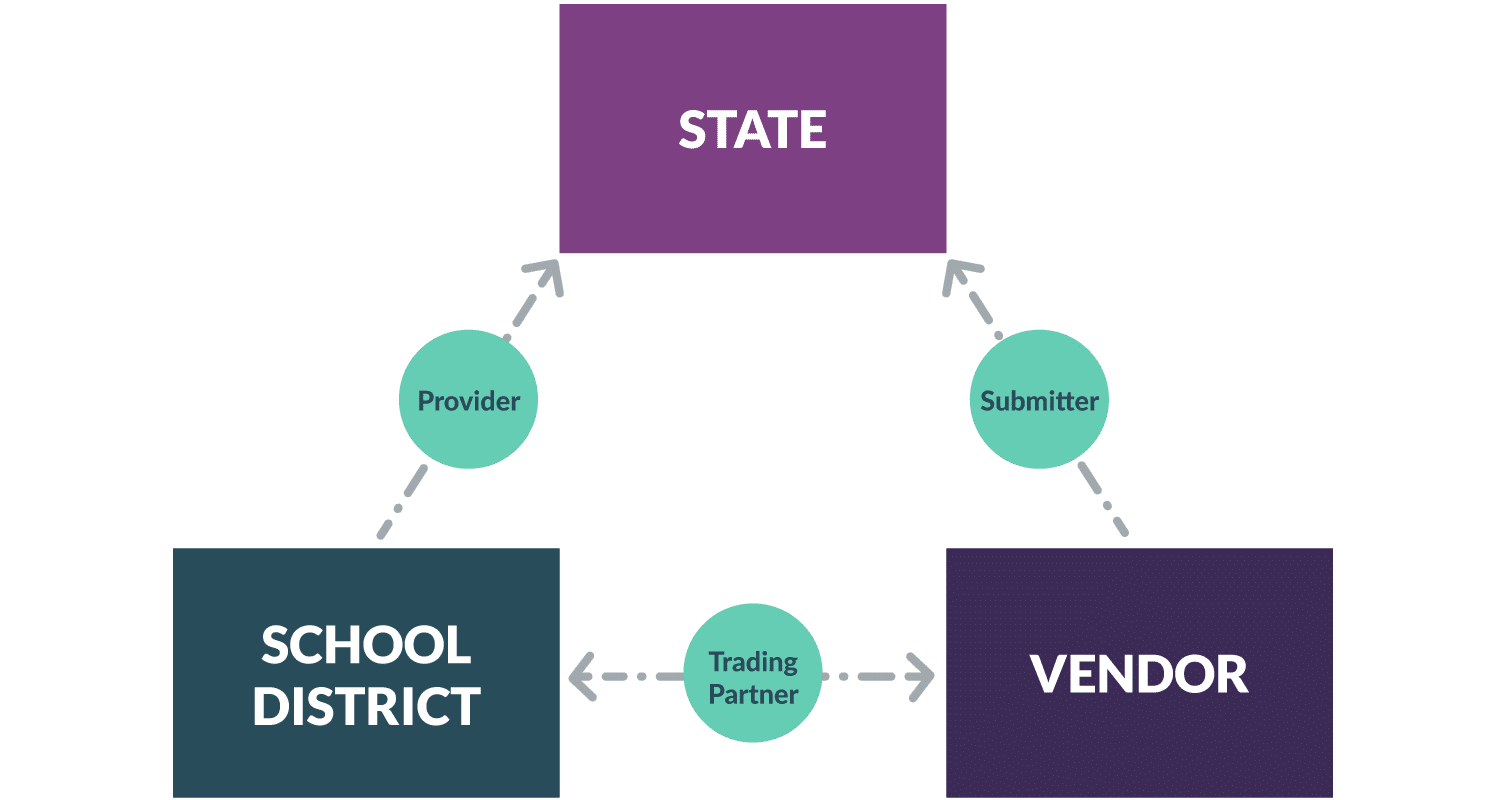
While all school districts are allowed to be Medicaid providers, each school district must apply to become a provider. This involves a lengthy application process with the state Medicaid agency. In addition, most districts choose to bill services through a third-party vendor — often called a submitter or clearinghouse: a private company that collects documentation and handles Medicaid transactions. Vendors must apply to become an approved submitter with each state and undergo an application and transaction testing process.
Once both entities are approved, school districts and vendors then declare their relationship to the state through a trading partner agreement that certifies the vendor is authorized to submit HIPAA-protected data to the state Medicaid agency on behalf of the school district.

Day-to-day claiming practices
Within a school district there are many different stakeholders that participate in the claiming process.
Health Service Provider(s): The largest group of stakeholders are the health care providers. These therapists, nurses, and mental health care providers who provide services to students in schools are responsible for accurately documenting those services and ensuring their documentation meets both Medicaid standards and licensing standards.
Medicaid Coordinator/Office: Depending on the size of the district, the Medicaid Coordinator or Medicaid Office is responsible for choosing which Medicaid-eligible services will be billed and is typically the primary liaison to the state Medicaid agency for regulatory questions and to the school district’s Medicaid billing vendor.
School District: The district is considered the provider and the claiming entity. All payments for services rendered at a school are submitted to the district as an organization and dispersed according to district policy. In some states, such as California, there are regulations around the usage and management of Medicaid revenue.
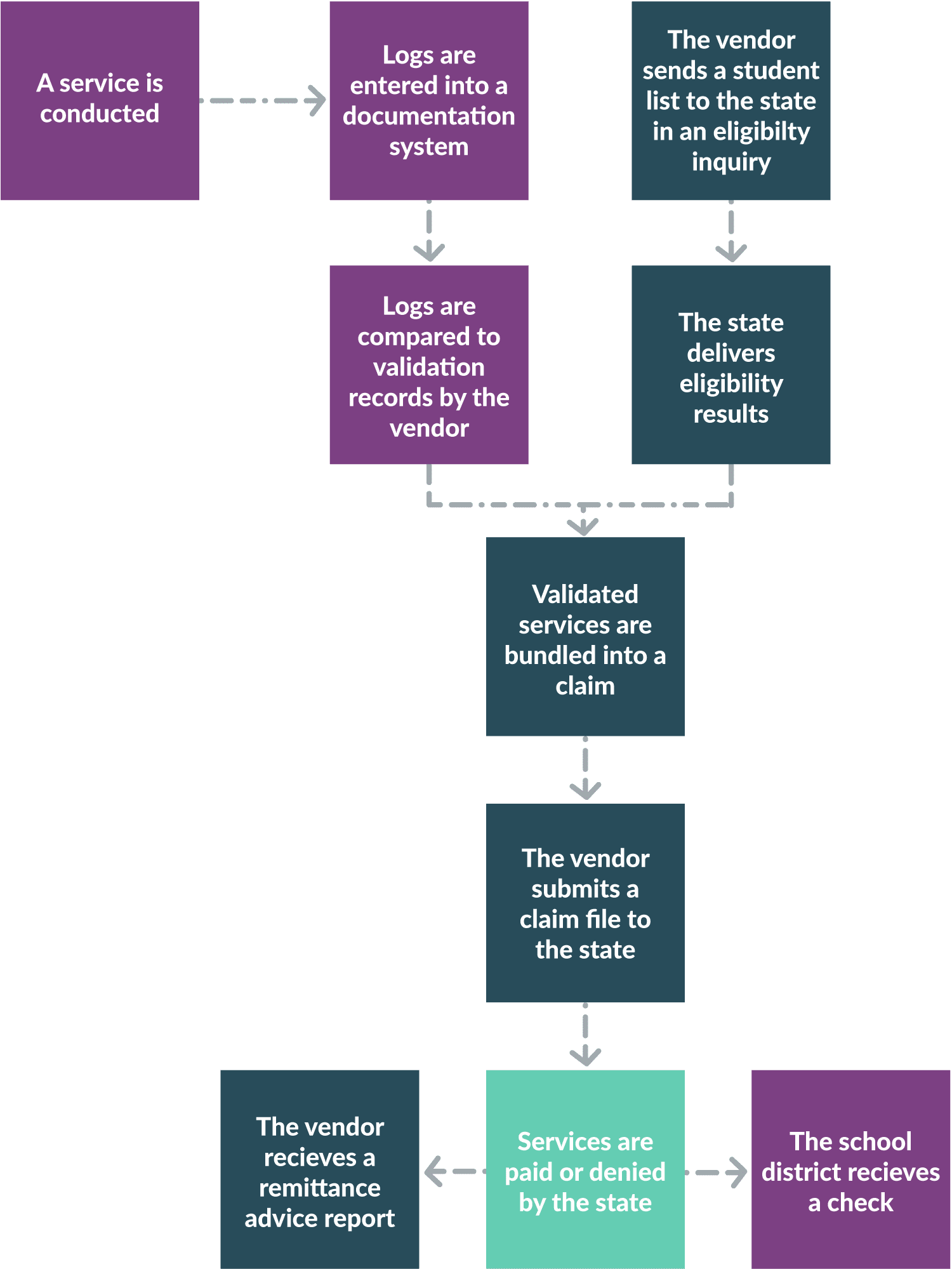
Documentation System: Most districts purchase an electronic web-based documentation system where providers can log their services electronically. This documentation system is often also a Medicaid billing software used to validate service logs for claiming by the Medicaid billing vendor, or can integrate with a Medicaid vendor to translate the documentation into billing information for submissions.
Medicaid Billing Vendor: The Medicaid billing vendor is the organization responsible for managing the billing program, from determining Medicaid eligibility to validating documentation entered by providers and generating Medicaid claim files that are sent to the state. Vendors also collect back remittance advice, which outlines the approval or denial of each service submitted, and the explanation of benefits. While vendors receive revenue information, the payment is sent directly to the school district as the provider.

Validations and audits
As district personnel document services given to students, districts must also prepare and maintain records to support all Medicaid billing. First and foremost is the proof of medical necessity: establishing the need for a medical service to address a diagnosed medical condition. In the wider medical world, this is determined by a doctor or other qualified health provider through an examination or evaluation. The need for ongoing therapy or treatment is defined in a plan of care that describes the condition and how the treatment will ameliorate that condition. Plans of care are often described through different terms, such as an individual health plan for nursing services.
Through IDEA, IEPs can be considered a plan of care and used to establish the medical necessity of the therapy or other health services mandated in the document. An IEP must include certain parameters to be considered a plan of care. These vary by state but commonly include:
- The proof of an evaluation by a qualified health care professional to determine a medical issue
- A defined frequency and scope of service delivery, usually to address a specific health goal
In addition to a valid IEP to support billing through the FFS program, school districts must also include records proving their providers meet the state licensure requirements, that parents have consented to allow Medicaid billing for their child, and in some cases a doctor’s sign-off of the IEP or plan of care.
You may enjoy this hand-picked content:
Medicaid does not collect or validate for this supporting data. It is expected that the school district, as the Medicaid provider, is reviewing each service and only submitting those that meet all criteria. State audits require all records surrounding any audited service be supplied to support billing.
Medicaid Expansion
In 2014, the federal government expanded Medicaid billing to include services beyond those written into an IEP. The implementation of this expansion is still ongoing as each state rewrites and submits new Medicaid state plans incorporating the new federal regulations into state practice.
Once a state plan is approved at the federal level, each state must rewrite its Medicaid regulations to define which additional programs can be considered valid for billing if they meet plan-of-care requirements. In Louisiana, for example, outside of IEPs, only nursing individual health plans were included for billing. In Colorado’s plan, the program type is not relevant as long as the program includes the plan-of-care requirements, which opens up billing for any service with a plan of care (for example, a Section 504 plan).
As states roll out regulations, you should pay close attention to where and when new services can be billed to increase the revenue that helps support service delivery as a whole.