



School-based Medicaid claiming programs enable districts to seek reimbursement through three distinct avenues: Fee-for-Service Billing (otherwise known as Direct Service Billing), School-Based Administrative Claiming, and Cost Reconciliation. Understanding the definitions of each program and how they are related are the first steps to understanding how the cost reconciliation process can impact your district’s revenue.
What is Fee-for-Service Medicaid billing?
Fee-for-Service (FFS) billing is the process of claiming for individual therapy or health sessions with students in a school setting. Sessions are bundled into claims and can be submitted throughout the year.
Reimbursable service types vary by state, but can include:
- Physician and nursing services
- Physical therapy
- Occupational therapy
- Speech therapy
- Audiological services
- Personal care services
- Transportation services
- Vision services
- Hearing services
- Mental health services
- Durable Medicaid equipment
- Case management
While payment schedules do vary from state to state, most districts can expect FFS payments within a month of claim submission. Payment totals are based on the procedure code identified by the provider in each session and are tied to a state-defined rate for that code.
Rates vary significantly. For example, individual speech therapy in Florida pays at $3.74 per 15 minutes. In Virginia, the rate is $31.91 per session. In both cases, the rate does not reflect the cost of service provision to the district.
What is School-Based Administrative Claiming?
School-Based Administrative Claiming (SBAC) is a quarterly process that allows districts to recoup funds based on the Medicaid administrative outreach and support activities conducted at the district. Claims are based on a quarterly time study that codes different types of professional activities from PTO to direct therapy time to educational services.
Districts begin the process by identifying the pool of personnel that conducts Medicaid outreach and support services. This pool is sampled using a Random Moment Time Study to determine the percentage of time spent on outreach and support services. The total percentage is then bundled into a quarterly claim along with personnel and other district expenditures. Districts receive a quarterly payment that reflects the portion of costs that were Medicaid related. However, according to CMS guidelines established in 2003, direct therapy costs are not included in the SBAC payment.1
What is Cost Reconciliation?
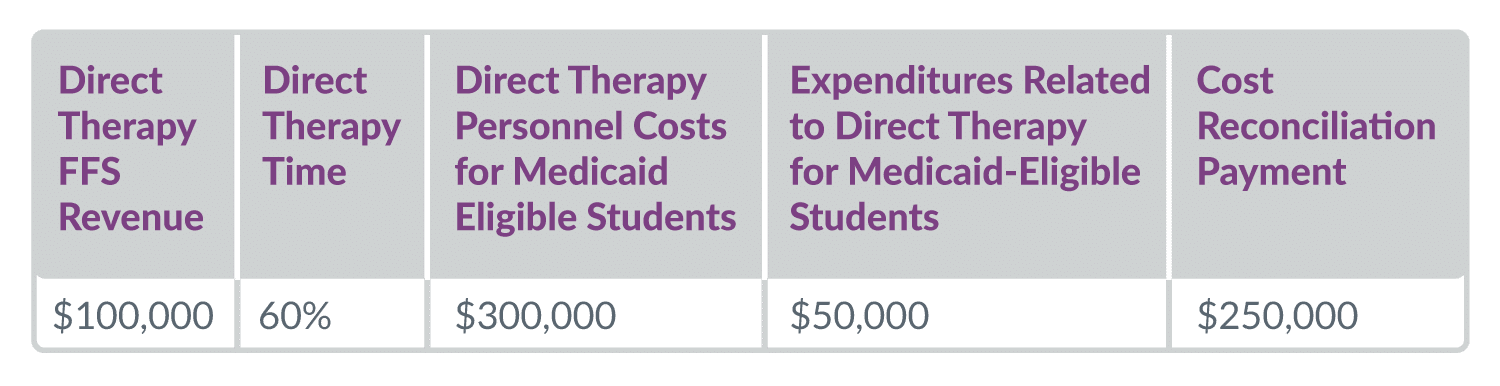
Cost Reconciliation (also known as Cost Settlement) is an annual process that allows districts to receive additional funding for direct therapy when the actual cost of service delivery exceeds that which was received in interim fee-for-service payments throughout the year. Not every state offers a cost reconciliation option, but in some states, Cost Reconciliation is required to ensure Medicaid reimbursement is consistent with the actual costs incurred in providing services.
The Cost Reconciliation submission-to-payment timeline is lengthy for two reasons: the report must be submitted after both the Fee-for-Service billing period and administrative claiming is completed for any fiscal year, and the report is audited prior to payment. Districts typically receive revenue 18 months to two years after services are delivered. Claiming requirements are similar to those used in SBAC claiming and some data pulls from the Random Moment Time Study process itself:
-
- The Random Moment Time Study process defines the overall percentage of time spent delivering direct therapy.
- The district is required to report:
- Total annual costs for personnel
- Total annual costs for district expenditures related to direct therapy for Medicaid-eligible students
- The total costs are then multiplied by the Medicaid Eligibility Rate within the IEP student population to determine the costs associated to direct therapy for Medicaid-eligible students.

Do I need to participate in Fee-for-Service claiming or Administrative Claiming to receive Cost Reconciliation funds?
In short, yes. Most states require some level of Fee-for-Service billing per quarter and service type for that personnel to be included in the cost report. In some cases, FFS billing must be maximized, or the districts overall revenue will be reduced in the cost report.2
In addition, because the cost report is based on percentages of direct therapy determined from the quarterly RMTS process, the RMTS is mandatory. While the district does not need to submit an SBAC claim from the RMTS process, these administrative costs for outreach and support services can be claimed through the SBAC program.
How can I maximize my Medicaid cost report for school-based services?
The best way to maximize your cost report is to review which costs your district is including as well as the sources of funding for those costs. In many instances, cost reporting maximization requires adjustments to your overall budgeting process.
Personnel costs
Providers that are funded through federal programs such as the Individuals with Disabilities Education Act (IDEA) cannot be included on a cost report. As you look to maximize your cost report, you should ensure that providers who conduct direct therapy are funded through local sources.
Expenditures
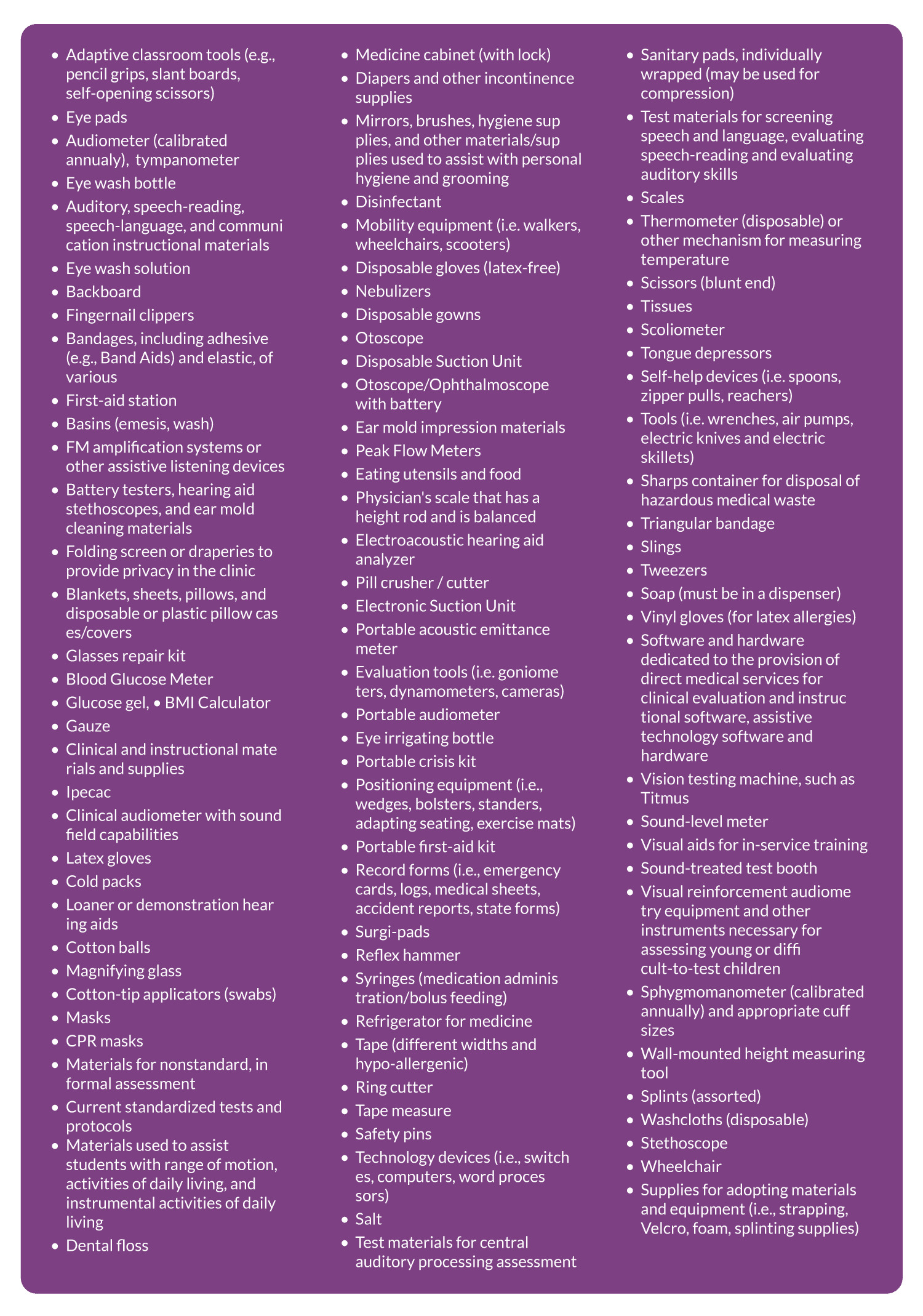
Districts can claim multiple types of expenditures for reimbursement, including large capital expenditures such as motorized wheelchairs or lifts. Costs to outfit buses with specialized medical equipment can also be claimed. In addition, the amortized cost of capital expenditures can be claimed annually.
Expenditures include not only the large capital expenses but also items like bandages or disinfectant. The below list captures the allowable costs in Texas for Medical supplies that can be claimed if they are used in support of Direct Medical Services:

Vendor fees for FFS claiming
The fees that vendors charge for supporting districts with documentation and FFS Medicaid claiming services can also be included in cost reports, depending on the state. In Virginia, for example, as long as the vendor fee is based on fixed pricing, this charge can be added to the cost report and reimbursed.
Medicaid Eligibility Rate
In some states, more than one type of Medicaid is allowed both for Fee-for-Service billing and Cost Reconciliation recoupment. When determining the Medicaid Eligibility Rate, you should analyze which types of Medicaid are acceptable for school-based claiming in your state. In some states, students who quality for State Children’s Health Insurance Program (SCHIP) meet the requirements to be claimed by schools.
What information should I have to back up my cost report?
Cost reports are not paid until they undergo an audit. You should have on hand:
- Transportation trip documentation
- IEP December 1 count
- Medicaid eligibility ratio
- Random Moment Time student pool personnel per quarter
- Random Moment Time Study results
You may enjoy this hand-picked content:
“My state does not have a Cost Reconciliation program”
You should petition your state Medicaid agency to develop a program! This is a long and tedious process for a state to undertake and would require the state agency submit a state plan amendment to the federal government for review, but it benefits school districts by bringing in more federal dollars to help provide health services to students. If Cost Reconciliation is not an option in your state, even if you maximize your Fee-for-Service claiming, state procedure code rates are not guaranteed to fully reimburse your costs.
Concluding thoughts
Cost Reconciliation is the best methodology to ensure that IDEA services are fully funded at the federal level by allowing districts to recoup exactly what they spent on the services they provided. However, the responsibility falls entirely on the district to claim every cost. We hope this guide will help your district examine your cost report with new eyes to ensure your Medicaid funding is maximized.
1 https://ahca.myflorida.com/medicaid/childhealthservices/schools/pdfs/School_District_Administrative_Claiming_Guide_2013.pdf
2 https://www.dmas.virginia.gov/files/links/156/Cost%20Report%20Instruction%20Guide.pdf